Medicare SGR sticker shock adds urgency to pay reform campaign - amednews.com
Tuesday, December 4, 2012
Medicare SGR sticker shock adds urgency to pay reform campaign - amednews.com
Sunday, December 2, 2012
Daily Kos: No, raising the Social Security retirement age is not a good idea
Daily Kos: No, raising the Social Security retirement age is not a good idea
res ipsa loquitor - the thing speaks for itself...

Monday, November 26, 2012
End-of-Life Health Care - NYTimes.com
End-of-Life Health Care - NYTimes.com
Fortunately, advance planning for end-of-life decisions has been going on for years and is continuing to spread despite the demagogy on the issue in 2009. There is good evidence that, done properly, it can greatly increase the likelihood that patients will get the care they really want. And, as a secondary benefit, their choices may help reduce the cost of health care as well.
Many people sign living wills that specify the care they want as death nears and powers of attorney that authorize relatives or trusted surrogates to make decisions if they become incapacitated. Those standard devices have been greatly improved in recent years by adding medical orders signed by a doctor — known as Physician Orders for Life Sustaining Treatment, or POLST — to ensure that a patient’s wishes are followed, and not misplaced or too vague for family members to be sure what a comatose patient would want.
Fifteen states, including New York, have already enacted laws or regulations to authorize use of these forms. Similar efforts are under development in another 28 states. The laws generally allow medical institutions to decide whether to offer the forms and always allow patients and families to decide voluntarily whether to use them.
With these physician orders, the doctor, or in some states a nurse practitioner or physician assistant, leads conversations with patients, family members and surrogates to determine whether a patient with advanced illness wants aggressive life-sustaining treatment, a limited intervention or simply palliative or hospice care.Sphere: Related Content
Tuesday, November 13, 2012
The Long Con: Mail-order conservatism | Rick Perlstein | The Baffler
The Long Con: Mail-order conservatism | Rick Perlstein | The Baffler
Ever wonder why right wing talk sponsors are so loyal?
In 2007, I signed on to the email lists of several influential magazines on the right, among them Townhall, which operates under the auspices of evangelical Stuart Epperson’s Salem Communications; Newsmax, the organ more responsible than any other for drumming up the hysteria that culminated in the impeachment of Bill Clinton; and Human Events, one of Ronald Reagan’s favorite publications. The exercise turned out to be far more revealing than I expected. Via the battery of promotional appeals that overran my email inbox, I mainlined a right-wing id that was invisible to readers who encounter conservative opinion at face value.
Subscriber lists to ideological organs are pure gold to the third-party interests who rent them as catchments for potential customers. Who better suits a marketing strategy than a group that voluntarily organizes itself according to their most passionately shared beliefs? That’s why, for instance, the other day I (and probably you) got an advertisement by way of liberal magazine The American Prospect seeking donations to Mercy Corps, a charity that helps starving children in the Third World. But back when I was getting emails every day from Newsmax and Townhall, the come-ons were a little bit different.
Dear Reader, I’m going to tell you something, but you must promise to keep it quiet. You have to understand that the “elite”would not be at all happy with me if they knew what I was about to tell you. That’s why we have to tread carefully. You see, while most people are paying attention to the stock market, the banks, brokerages and big institutions have their money somewhere else . . . [in] what I call the hidden money mountain . . . All you have to know is the insider’s code (which I’ll tell you) and you could make an extra $6,000 every single month.
Soon after reading that, I learned of the“23-Cent Heart Miracle,” the one “Washington, the medical industry, and drug companies REFUSE to tell you about.” (Why would they? They’d just be leaving money on the table: “I was scheduled for open heart surgery when I read about your product,” read one of the testimonials. “I started taking it and now six months have passed and I haven’t had open-heart surgery.”) Then came news of the oilfield in the placenta.
“Dear NewsMax Reader,” this appeal began, leaving no doubt that whatever trust that publication had built with its followers was being rented out wholesale. “Please find below a special message from our sponsor, James Davidson, Editor of Outside the Box. He has some important information to share with you.”
Here’s the information in question: “If you have shied away from profiting from the immense promise of stem cells to treat disease because of moral concern over extracting stem cells from fetal tissue, pay close attention. You can now invest with a clear conscience. An Israeli entrepreneur, Zami Aberman, has discovered‘an oilfield in the placenta.’ His little company, Pluristem Life Systems (OTCBB: PLRS) has made a discovery which is potentially more valuable than Prudhoe Bay.”
Davidson concluded by proposing the lucky investor purchase a position of 83,000 shares of PLRS for the low, low price of twelve cents each. If you act now, Davidson explained, your $10,000 outlay “could bring you a profit of more than a quarter of a million dollars.”
Not long after I let the magic of the placenta-based oilfield sink in, I got another pitch, this one courtesy of the webmasters handling the Human Events mailing list and headed “The Trouble with Get-Rich-Quick Schemes.” Perhaps I’m a little gullible myself; for a couple of seconds, I believed the esteemed Reagan-era policy handbook might be sending out a useful consumer advisory to its readers, an investigative guide to the phony get-rich-quick schemes caroming around the right-leaning opinion-sphere. But that hasty assumption proved sadly mistaken, presuming as it did that the proprietors of outfits likeHuman Events respect their readers. Instead, this was a come-on for something called“INSTANT INTERNET INCOME”—the chance at last to “put an end to your financial worries . . . permanently erase your debts . . . pay cash for the things you want . . . create a secure, enjoyable retirement for yourself . . . give your family the abundant lifestyle they so richly deserve.”Sphere: Related Content
Monday, November 12, 2012
Hurricane Sandy: beware of America's disaster capitalists | Naomi Klein | Comment is free | The Guardian
The prize for shameless disaster capitalism, however, surely goes to rightwing economist Russell S Sobel, writing in a New York Times online forum. Sobel suggested that, in hard-hit areas, Federal Emergency Management Agency (Fema) should create "free-trade zones – in which all normal regulations, licensing and taxes [are] suspended". This corporate free-for-all would, apparently, "better provide the goods and services victims need".
Yes, that's right: this catastrophe, very likely created by climate change – a crisis born of the colossal regulatory failure to prevent corporations from treating the atmosphere as their open sewer – is just one more opportunity for further deregulation. And the fact that this storm has demonstrated that poor and working-class people are far more vulnerable to the climate crisis shows that this is clearly the right moment to strip those people of what few labour protections they have left, as well as to privatise the meagre public services available to them. Most of all, when faced with an extraordinarily costly crisis born of corporate greed, hand out tax holidays to corporations.
The flurry of attempts to use Sandy's destructive power as a cash grab is just the latest chapter in the very long story I have called the The Shock Doctrine. And it is but the tiniest glimpse into the ways large corporations are seeking to reap enormous profits from climate chaos.
One example: between 2008 and 2010, at least 261 patents were filed or issued relating to "climate-ready" crops – seeds supposedly able to withstand extreme conditions such as droughts and floods; of these patents close to 80% were controlled by just six agribusiness giants, including Monsanto and Syngenta. With history as our teacher, we know that small farmers will go into debt trying to buy these new miracle seeds, and that many will lose their land.Sphere: Related Content
Sunday, November 11, 2012
What do top hospitals have in common? Not as much as you think.
What do top hospitals have in common? Not as much as you think.
Researchers at the Atlas looked at how the top 23 academic medical centers, as ranked by U.S. News and World Report, provide care to their patients. Their results show huge variations in how the very best hospitals care for their sickest patients.
A patient at New York Presbyterian Hospital can expect to spend 20 days in the hospital during the last six months of life. The average Mayo Clinic patient would have 10 days in the hospital over the same time span.
At the University of Utah, the average patient sees 20 doctors during the last six months of life. At the Cedars-Sinai Hospital in California, that number is 73 physicians.
A patient at UCLA’s Ronald Reagan Hospital is three times as likely to have a fall or injury while in the hospital than one at Cedars Sinai, also in Los Angeles.
“We know these differences cannot be explained by the prevalence of diseases,” Goodman says. “Yes, populations differ. Those are small differences we see compared to the dramatic differences in care.”Sphere: Related Content
Tuesday, October 30, 2012
PLOS ONE: Healthcare Reform and the Next Generation: United States Medical Student Attitudes toward the Patient Protection and Affordable Care Act
Of medical students surveyed, 94.8% agreed that the existing United States healthcare system needs to be reformed, 31.4% believed the PPACA will improve healthcare quality, while 20.9% disagreed and almost half (47.7%) were unsure if quality will be improved. Two thirds (67.6%) believed that the PPACA will increase access, 6.5% disagreed and the remaining 25.9% were unsure. With regard to containing healthcare costs, 45.4% of participants indicated that they are unsure if the provisions of the PPACA will do so. Overall, 80.1% of respondents indicated that they support the PPACA, and 78.3% also indicated that they did not feel that reform efforts had gone far enough. A majority of respondents (58.8%) opposed repeal of the PPACA, while 15.0% supported repeal, and 26.1% were undecided.
Conclusion
The overwhelming majority of medical students recognized healthcare reform is needed and expressed support for the PPACA but echoed concerns about whether it will address issues of quality or cost containment.Sphere: Related Content
Monday, October 29, 2012
The price of Medicaid expansion opt-outs: $53.3 billion
The price of Medicaid expansion opt-outs: $53.3 billion
The Supreme Court decided way back in June that the health law’s expansion of Medicaid was optional rather than required. That decision, it appears, comes with a hefty price tag: $53.3 billion.
The National Association of Public Hospitals estimates that, in light of the decision, the United States will spend as much as $53.3 billion more on bills that go unpaid by the uninsured. Their analysis uses data from the Congressional Budget Office, which estimates that six million to10 million fewer Americans will gain insurance through Medicaid after the Supreme Court decision.
“Congress certainly didn’t foresee this level of uninsured and uncompensated care when it enacted the ACA,” says NAPH president Bruce Seigel.
Keep in mind, this isn’t necessarily $53.3 billion in new spending. It’s more like a cost shift. Those who would have had their bills paid by the federal government (under Medicaid) could now have the costs covered by local governments and hospitals, which tend to foot the bill for many of the health care services that go unpaid.
The Congressional Budget Office estimates that, over the course of a decade, states opting out of the Medicaid expansion – and not drawing down funds from Washington – will save the federal government $84 billion.
It’s also a cost shift to those with private insurance, as hospitals charge a bit more to clients with coverage to recoup their losses on the uninsured. One study estimated that cost shifting raises annual insurance premiums by as much as 1.7 percent, or $80 annually.Sphere: Related Content
Why I Am Pro-Life - NYTimes.com
Why I Am Pro-Life - NYTimes.com
In my world, you don’t get to call yourself “pro-life” and be against common-sense gun control — like banning public access to the kind of semiautomatic assault rifle, designed for warfare, that was used recently in a Colorado theater. You don’t get to call yourself “pro-life” and want to shut down the Environmental Protection Agency, which ensures clean air and clean water, prevents childhood asthma, preserves biodiversity and combats climate change that could disrupt every life on the planet. You don’t get to call yourself “pro-life” and oppose programs like Head Start that provide basic education, health and nutrition for the most disadvantaged children. You can call yourself a “pro-conception-to-birth, indifferent-to-life conservative.” I will never refer to someone who pickets Planned Parenthood but lobbies against common-sense gun laws as “pro-life.”
“Pro-life” can mean only one thing: “respect for the sanctity of life.” And there is no way that respect for the sanctity of life can mean we are obligated to protect every fertilized egg in a woman’s body, no matter how that egg got fertilized, but we are not obligated to protect every living person from being shot with a concealed automatic weapon. I have no respect for someone who relies on voodoo science to declare that a woman’s body can distinguish a “legitimate” rape, but then declares — when 99 percent of all climate scientists conclude that climate change poses a danger to the sanctity of all life on the planet — that global warming is just a hoax.
The term “pro-life” should be a shorthand for respect for the sanctity of life. But I will not let that label apply to people for whom sanctity for life begins at conception and ends at birth. What about the rest of life? Respect for the sanctity of life, if you believe that it begins at conception, cannot end at birth. That radical narrowing of our concern for the sanctity of life is leading to terrible distortions in our society.Sphere: Related Content
Medicaid on the Ballot - NYTimes.com
Medicaid on the Ballot - NYTimes.com
But one thing is clear: If [Romney] wins, Medicaid — which now covers more than 50 million Americans, and which President Obama would expand further as part of his health reform — will face savage cuts. Estimates suggest that a Romney victory would deny health insurance to about 45 million people who would have coverage if he lost, with two-thirds of that difference due to the assault on Medicaid.
....
So, about coverage: most Medicaid beneficiaries are indeed relatively young (because older people are covered by Medicare) and relatively poor (because eligibility for Medicaid, unlike Medicare, is determined by need). But more than nine million Americans benefit from both Medicare and Medicaid, and elderly or disabled beneficiaries account for the majority of Medicaid’s costs. And contrary to what you may have heard, the great majority of Medicaid beneficiaries are in working families.
For those who get coverage through the program, Medicaid is a much-needed form of financial aid. It is also, quite literally, a lifesaver. Mr. Romney has said that a lack of health insurance doesn’t kill people in America; oh yes, it does, and states that expand Medicaid coverage show striking drops in mortality.
So Medicaid does a vast amount of good. But at what cost? There’s a widespread perception, gleefully fed by right-wing politicians and propagandists, that Medicaid has “runaway” costs. But the truth is just the opposite. While costs grew rapidly in 2009-10, as a depressed economy made more Americans eligible for the program, the longer-term reality is that Medicaid is significantly better at controlling costs than the rest of our health care system.
How much better? According to the best available estimates, the average cost of health care for adult Medicaid recipients is about 20 percent less than it would be if they had private insurance. The gap for children is even larger.Sphere: Related Content
Sunday, October 28, 2012
U.S. to Sponsor Health Insurance Plans Nationwide - NYTimes.com
U.S. to Sponsor Health Insurance Plans Nationwide - NYTimes.com
The Obama administration will soon take on a new role as the sponsor of at least two nationwide health insurance plans to be operated under contract with the federal government and offered to consumers in every state.
These multistate plans were included in President Obama’s health care law as a substitute for a pure government-run health insurance program — the public option sought by many liberal Democrats and reviled by Republicans. Supporters of the national plans say they will increase competition in state health insurance markets, many of which are dominated by a handful of companies.
The national plans will compete directly with other private insurers and may have some significant advantages, including a federal seal of approval. Premiums and benefits for the multistate insurance plans will be negotiated by the United States Office of Personnel Management, the agency that arranges health benefits for federal employees.
Walton J. Francis, the author of a consumer guide to health plans for federal employees, said the personnel agency had been “extraordinarily successful” in managing that program, which has more than 200 health plans, including about 20 offered nationwide. The personnel agency has earned high marks for its ability to secure good terms for federal workers through negotiation rather than heavy-handed regulation of insurers.Sphere: Related Content
Saturday, October 27, 2012
Partisanship guides American attitudes on health-care reform - DC Breaking Local News Weather Sports FOX 5 WTTG
Partisanship guides American attitudes on health-care reform
Predictably, individual views on the law's effects -- for good or ill -- also fell along party lines. Twenty-two percent of Democrats say the ACA has had an overall positive effect on their lives, compared to only 4 percent of Republicans. Similarly, 42 percent of Republicans deem the overall effect as negative, compared with 9 percent of Democrats.
"Republicans are much more likely to see negative effects of the ACA, including some effects (increased taxes or a decline in quality of care) which are almost certainly not linked to the Affordable Care Act," Taylor said. "Democrats tend to see positive effects that [also] may be real or imagined."
Although the poll numbers appear mixed, Ron Pollack, executive director of Families USA in Washington, D.C., believes that public attitudes will lean more toward the positive as 2014 approaches and more of the law's key elements are enacted.Sphere: Related Content
The Best of CBPP Graphs: Guideposts on the Road Back to Factville | Jared Bernstein | On the Economy
The Best of CBPP Graphs: Guideposts on the Road Back to Factville | Jared Bernstein | On the Economy
A nice collection of graphics, including this great one, from CBPP courtesy of Jared Bernstein...

Tuesday, October 23, 2012
Obamacare Is Not Causing Small Businesses To Drop Their Employees' Coverage | ThinkProgress
Obamacare Is Not Causing Small Businesses To Drop Their Employees' Coverage | ThinkProgress
And a new study assuages similar fears that small business owners might drop coverage for their employees before Obamacare takes effect in order to avoid being hit with crippling expenses. The Midwest Business Group on Health surveyed businesses across 16 states, ranging in size from small companies with fewer than 1,000 employees to larger corporations that employ more than 5,000, and found “little indication that employers plan to drop health care coverage.”
As Forbes reports, while employers understand that they may want to adjust the scope of their health benefits plans, they are not anticipating the need to drop coverage for their employees because of the health reform law’s implementation...Sphere: Related Content
Orthopedic Group in Philly lays down big bet for Romney
PhillyDeals: Small-business owners plan to delay hiring process until after election
Rothman for Romney
Doctors who staff the Philadelphia-based Rothman Institute chain of orthopedic clinics were, as a group, the "top contributors to Mitt Romney's Republican campaign for the third quarter of 2012," the Washington Post reports, citing Federal Election Commission data.
Contributions to a pro-Romney fund from 65 Rothman doctors on Sept. 17 totaled $751,000. The second-largest Romney-donor employer group for that period worked for private-equity investors Kohlberg Kravis Roberts, which gave $480,000.
Why do these bone men want to dump President Obama? Rothman spokesman Richard Cushman declined to comment when my colleague Harold Brubaker asked.I know, I know! They have huge incomes and don't want them to change one little bit. Sphere: Related Content
Settlement Eases Rules for Some Medicare Patients - NYTimes.com
Settlement Eases Rules for Some Medicare Patients - NYTimes.com
This is pretty huge, actually!
In a proposed settlement of a nationwide class-action lawsuit, the administration has agreed to scrap a decades-old practice that required many beneficiaries to show a likelihood of medical or functional improvement before Medicare would pay for skilled nursing and therapy services.
Under the agreement, which amounts to a significant change in Medicare coverage rules, Medicare will pay for such services if they are needed to “maintain the patient’s current condition or prevent or slow further deterioration,” regardless of whether the patient’s condition is expected to improve.
Federal officials agreed to rewrite the Medicare manual to make clear that Medicare coverage of nursing and therapy services “does not turn on the presence or absence of an individual’s potential for improvement,” but is based on the beneficiary’s need for skilled care.Sphere: Related Content
Disparity in pay divides doctors - The Washington Post
Disparity in pay divides doctors - The Washington Post
A nice summary of pay disparity in medicine.
Recently, a medical student confided in me a thought that few in our profession would dare say aloud: “We may have come to medical school to help people, but we choose our specialty careers based on potential salaries.”
This in part explains why the most-prized residencies are in fields such as dermatology and radiology, whose procedures generate high fees. According to a physician survey by the Medical Group Management Association, the median income of specialists is nearly twice that of primary-care physicians — $384,000 vs. $212,000. The highest-paid gastroenterologists make about $846,000 a year; the highest-paid internists make about $352,000.
As in most professions, it has long been true in medicine that specialists earn more than generalists. They train longer and in many cases pay higher insurance rates, but these factors don’t fully explain the chasm. We’ve now reached a critical point where the income disparity is harming the general population.Sphere: Related Content
JAMA- AIM | Physicians' Opinions About Reforming ReimbursementResults of a National SurveyReforming Reimbursement
Results
The response rate was 48.5% (n = 1222). Four of 5 physicians (78.4%) indicated that under Medicare, some procedures are compensated too highly and others are compensated at rates insufficient to cover costs. Incentives were the most frequently supported reform option (49.1%), followed by shifting payments (41.6%) and bundling (17.2%). Shifting payments and bundling were more commonly supported by generalists than by other specialists. There was broad support for increasing pay for generalists (79.8%), but a proposal to offset the increase with a 3% reduction in specialist reimbursement was supported by only 39.1% of physicians.
Conclusions
Physicians are dissatisfied with Medicare reimbursement and show little consensus for major proposals to reform reimbursement. The successful adoption of payment reform proposals may require a better understanding of physicians' concerns and their willingness to make tradeoffs.Sphere: Related Content
Saturday, October 20, 2012
Health care for all: Expanding Medicaid would save lives, suffering and money - Pittsburgh Post-Gazette - Printer friendly
Health care for all: Expanding Medicaid would save lives, suffering and money - Pittsburgh Post-Gazette - Printer friendly
My Piece on Medicaid expansion from the P-G:
Health care for all: Expanding Medicaid would save lives, suffering and money
As someone whose profession takes a strong position in favor of universal access to health care, I have a hard time saying anything but, "What a great problem to have!" It turns out to not even be a problem.
Massachusetts did this many years ago, as we are being frequently reminded, and the results are in. Use of emergency rooms is down, waiting times to see a primary care doctor are essentially unchanged and there has been a vast expansion in the use of preventive services: mammograms, colon cancer screens and prenatal care, for instance. Doctors and the people of Massachusetts overwhelmingly favor continuation of their program, and they are now proceeding to the really hard part: getting costs under control. Stay tuned!
An even more interesting experiment is being conducted in Oregon via an unhappy accident. Due to a shortage of funds, Medicaid eligibility was determined by lottery, creating a natural experiment of haves and have-nots. In the first year, those who were enrolled were 70 percent more likely to have a usual source of care, were 55 percent more likely to see the same doctor over time, received 30 percent more hospital care and received 35 percent more outpatient care, and much more.
Every doctor you know can tell you stories about how the lack of access to health insurance and health care has injured a patient's health, life, limbs, finances or all of the above. I've had patients who work full time in jobs that fall far short of the American dream. They get by, but they can't afford health insurance.
There's the cabbie who recognizes his diabetes and determines to work harder and longer so he can buy insurance before he is stricken with the label even worse than diabetes: preexisting condition! He doesn't make it and ends up in the ICU with diabetic ketoacidosis.
There's the construction worker who has a controllable seizure disorder that goes uncontrolled. He ends up in the ICU multiple times.
There's the woman who stays home to care for her dying mother and loses her insurance along with her job. When she finally gets to a doctor for herself, her cancer is far advanced.
So, for me and my profession, the most expansion for the most people is a best-case scenario. But others see expanding health insurance only through a short-term budgetary lens and consider covering nearly everyone a worst case.
For one thing, this view ignores the incredible deal states get when they accept Medicaid expansion. According to the Kaiser Foundation, by 2019 Pennsylvania would add about 482,000 new enrollees; another 282,000 who are eligible but don't know it would come into the program. That's more than three-quarters of a million people with access to care.
Critics point to the potential cost to the state of more than a billion dollars over six years. That's a lot of money, but the federal government would pay more than $17 billion -- over 94 percent of the cost. Furthermore, the additional billion would be only 1.4 percent more than Pennsylvania's currently scheduled spending over that period. Even in a best-case scenario, with insurance for an additional 1.1 million Pennsylvanians, this figure would rise to only 2.7 percent.
One can choose to focus on the costs to the state and federal governments, but we spend many of those dollars already on the wrong end of the care continuum. Our governments already pay for patients who cannot pay for themselves, largely by cutting big checks to hospitals.
You can take care of a lot of diabetic cabbies for a lot of years for the cost of a stay in the ICU. Just because the costs don't show up as a line item in a government budget -- it could be labeled "Exorbitant Amounts of Money for Preventable Complications and Deaths" -- doesn't mean we don't pay them.
A frequent talking point against expanding access to health care, "You can always go to an emergency room," is actually dead on. Literally.
The law requires emergency rooms to treat and stabilize patients even if they have no means to pay. But no emergency room does cancer screening. Or prenatal care. No emergency room manages diabetes. Or congestive heart failure. As a result, many people don't seek treatment until they are nearly dead.
Patients forgoing care or medicines because they can't afford them simply shifts the costs from keeping people healthy to our extremely expensive system of "rescue care." And remember, Massachusetts' early experience and Oregon's current experiment are showing the benefits to the entire system of getting people taken care of before they need an ER or ICU.
Not long ago, expanding access to health care was a nonpartisan goal. As recently as 2007, a bipartisan group of U.S. senators, including Republicans Jim DeMint and Trent Lott, wrote a letter to then-President George W. Bush pointing out that our health care system was in urgent need of repair. "Further delay is unacceptable as costs continue to skyrocket, our population ages and chronic illness increases. In addition, our businesses are at a severe disadvantage when their competitors in the global market get health care for 'free.' "
Their No. 1 priority? "Ensure that all Americans would have affordable, quality, private health coverage, while protecting current government programs. We believe the health care system cannot be fixed without providing solutions for everyone. Otherwise, the costs of those without insurance will continue to be shifted to those who do have coverage."
Medicaid expansion, as well of the rest of the new health care law, represents our best effort so far in reaching these once-bipartisan goals. Pennsylvanians deserve an expansion of health insurance and health care, a healthier state, a healthier workforce and to continue the journey toward my profession's goal: excellent, affordable health care for all.
Christopher M. Hughes practices intensive care and hospice medicine in Pittsburgh and is the Pennsylvania director of Doctors for America (www.drsfor america.org).
First Published October 4, 2012 12:00 am Sphere: Related Content
How Much Do People Pay in Taxes?
How Much Do People Pay in Federal Taxes? | pgpf.org
These top two graphics do NOT include state and local sales tax, nor property taxes, both of which tend to be very regressive, stacking onto the left sides of these graphs very significantly. Scroll down for TOTAL tax burden.
Effective tax rates: individual income and payroll taxes combined
Percent of cash income
Percent of cash income

SOURCE: TPC, Table T12‐0018 Effective Federal Tax Rates by Cash Income Percentile; 2011, February 2012. Compiled by PGPF.
NOTE: *Individual income tax rates for the lowest and second lowest quintiles are negative and are netted against the payroll tax rate. A quintile is one fifth of the population. Calculations assume that employees also pay the employer portion of payroll taxes in the form ofreduced wages. The breaks are (in 2011 dollars): 20% $16,812; 40% $33,542; 60% $59,486; 80% $103,465; 90% $163,173; 95%$210,998; 99% $532,613; 99.9% $2,178,886.
Effective tax rates: income, payroll, corporate and estate taxes combined
Percent of cash income
Percent of cash income

SOURCE: TPC, Table T12‐0018 Effective Federal Tax Rates by Cash Income Percentile; 2011, February 2012. Compiled by PGPF.
NOTE: *Individual income tax rates for the lowest and second lowest quintiles are negative and are netted against the payroll tax rate. A quintile is one fifth of the population. Calculations assume that employees also pay the employer portion of payroll taxes in the form ofreduced wages. The breaks are (in 2011 dollars): 20% $16,812; 40% $33,542; 60% $59,486; 80% $103,465; 90% $163,173; 95% $210,998; 99% $532,613; 99.9% $2,178,886.
Total tax burden, from the Center for Tax Justice, via the NY Times Economix Blog:

Federal individual income tax rates for married couples, filing jointly, 2012
| Taxable Income | Marginal Tax Rate | Income Tax Owed | |
|---|---|---|---|
| Over | But not over | ||
| $0 | $17,400 | 10% | 10% of taxable income |
| $17,400 | $70,700 | 15% | 10% x $17,400 = $1,740 plus 15% x income over $17,400 |
| $70,700 | $142,700 | 25% | $1,740 + 15% x (70,700 ‐17,400) = $9,735 plus 25% x income over $70,700 |
| $142,700 | $217,450 | 28% | $9,735 + 25% x (142,700 ‐ 70,700) = $27,735 plus 28% x income over $142,217 |
| $217,450 | $388,350 | 33% | $ 27,735 + 28% x ( 217,450 ‐ 142,700) = $ 48,665 plus 33% x income over $217,450 |
| $388,350 | 35% | $48,665 + (388,350 – 217,450) = $105,062 plus 35% x income above $388,350 | |
SOURCE: Joint Committee on Taxation, Overview Of The Federal Tax System As In Effect For 2012 (JCX 18‐12), February 24, 2012.
But note that these tax rates, particularly the top marginal rate are incredibly low in historical context, as are the tax burden on the wealthiest:

Wednesday, October 17, 2012
Health Care Policy under President Romney — NEJM
Health Care Policy under President Romney — NEJM
Also uncertain is whether a Romney administration would seek repeal of the $716 billion in Medicare savings that would be used to finance about half the ACA's cost. Though Romney has committed to repealing these savings, his running mate, Congressman Paul Ryan (R-WI), incorporated them into his House budget resolutions in 2011 and 2012, with overwhelming support from the House Republican Caucus.4 Rescinding these savings would advance the insolvency of the Medicare Part A Hospital Insurance Trust Fund from 2024 to 2016 and trigger an average increase of $323 in the premiums paid by most Medicare beneficiaries between 2013 and 2022. Romney has pledged not to change Medicare for current enrollees.2 However, premium increases for future enrollees, plus the elimination of ACA-created Medicare benefits such as no-cost preventive services, will test that pledge.
Romney and the Republican National Platform also endorse Ryan's proposal to convert Medicare from a defined-benefit to a defined-contribution program.2,4 Under this plan, new senior and disabled Medicare enrollees (beginning in 2023) would receive a capped subsidy (“premium support”) to purchase individual coverage from competing private and public (traditional Medicare) health plans.2,4 Romney also proposes to increase Medicare's eligibility age from 65 to 67 and to provide less premium support to wealthier seniors.2 These changes would reduce future federal Medicare spending beginning in 2023 and would shift growing costs to beneficiaries.
Romney also endorses Ryan's proposal to modify the federal–state Medicaid partnership by turning the program into block grants and capping the federal contribution.2,4 The corresponding budget resolution calls for cuts (beyond those effected by ACA repeal) of $810 billion over 10 years (2013 through 2022).4 These cuts would mean curtailing benefits, reducing provider payments, tightening eligibility, shrinking enrollee rolls, and swelling the ranks of the uninsured by 14 million to 27 million people, according to the Kaiser Commission on Medicaid and the Uninsured.5 Though Romney outlines countermeasures such as state-sponsored high-risk pools and insurance subsidies, both options are costly and contingent on flush state coffers.Sphere: Related Content
Ear reconstruction service and rationing, US v UK
Ear reconstruction service
Recently I found out, by accident (ask me in person how), that my local BC/BS carrier only pays for ear reconstruction if hearing is an issue, not for cosmetics. I was curious about whether England's NHS would be so, well, "rationing" of care. Turns out, they are OK with it. But remember, your insurer never denies the procedure, they just deny the payment! There, feel better?
Ear reconstruction is considered as one of the most challenging operations in plastic surgery. It is usually undertaken in specialist centres, where, with the appropriate training and case availability it is possible to attain excellent results. The majority of plastic surgeons see 1-2 cases per year. In view of the rarity of the condition specialist centres such as the Royal Free Hospital have developed to provide a national tertiary referral service. Ear reconstruction is requested by two main groups of patients: those who have an underdeveloped ear at birth (a condition known as microtia) and those who have lost a normal ear through trauma, disease or previous surgery.Sphere: Related Content
A 20-Year Low in U.S. Carbon Emissions - NYTimes.com
A 20-Year Low in U.S. Carbon Emissions - NYTimes.com
For everyone with those yard signs saying "Stop the war on coal - fire Obama"
The war on coal is being fought by basic economics - cheaper, more efficient natural gas is kicking coal's butt. Obama has nothing to do wiuth it and neither would Romney.
Energy-related carbon dioxide emissions in the United States from January through March were the lowest of any recorded for the first quarter of the year since 1992, the federal Energy Information Administration reports.
The agency attributed the decline to a combination of three factors: a mild winter, reduced demand for gasoline and, most significant, a drop in coal-fired electricity generation because of historically low natural gas prices. Whether emissions will continue to drop or begin to rise again, however, remains to be seen, experts said Friday.
“While this is a positive step, we shouldn’t just say, ‘Oh, we’ve got plenty of natural gas, we can just switch to that, problem solved,’ and move on,” said Jay Apt, the director of the Carnegie Mellon Electricity Industry Center, who was not involved in compiling the study.
Carbon dioxide emissions from energy consumption totaled 1.34 billion metric tons in the first quarter, down nearly 8 percent from a year earlier, the Energy Information Administration said.
Although natural gas is a more efficient fossil fuel than coal, burning it still produces carbon dioxide emissions. One of its strengths is that it produces more kilowatts of power than the equivalent amount of coal and it provides more energy for each carbon dioxide molecule emitted into the atmosphere. This so-called carbon efficiency is a crucial factor that allows scientists to project carbon dioxide emissions, with more efficient energy sources contributing less to climate change than the more inefficient sources.
Coal-fired electric power generation puts out about twice the amount of carbon dioxide — around 2,000 pounds for every megawatt hour generated — than electricity generated by burning natural gas. But that is still about 1,100 pounds per megawatt hour for electricity from natural gas. Scientists suggest the United States needs to reduce emissions to around 350 to 400 pounds per megawatt hour to stabilize atmospheric concentrations.
The extraction of large natural gas deposits in the Marcellus Shale has contributed to the rise of inexpensive natural gas, causing prices to decline in the last four years and making it a far cheaper option than burning coal. In 2005, coal accounted for half of all electricity generated in the country. But the embrace of natural gas, which now accounts for about 30 percent of electricity generation, has caused coal’s share to retreat to 34 percent, a 40-year low.
Additionally...
A November 2010 EIA report on power plant operating costs — the latest data available — found that a typical coal-fired plant costs $2,800 to $3,200/kilowatt of generation capacity, while a modern natural gas-fired plant costs around $1,000/kilowatt.
Combine significantly cheaper fuel costs and leaner operating costs, and electricity from a convention coal fired plant costs 9.5 cents/per kilowatt hour to produce, compared with 6.6 cents at a conventional modern gas plant, according to EIA's Energy Outlook 2011.
-------------------
Of the nation's 600 coal-fired power plants — roughly 44 percent of U.S. power generation capacity — most are in the Midwest, with Ohio, Indiana, Pennsylvania and Illinois home to half of them. Some of those states also happen to be home to the Marcellus shale formation.
The attraction of natural gas comes at a time many coal-fired plants have reached the end of their life span.
According to DB Climate Advisors and the Electric Power Research Institute, an industry lab and think tank, nearly 60gw of coal-fired generation assets are antiquated, some of it up to 80 years old.
"They should have been put out of their misery long ago," says DB's Fulton.
Sphere: Related Content
Monday, October 15, 2012

Romney’s Medicaid shell game - Boston.com
Romney’s Medicaid shell game - Boston.com
Mitt Romney is lambasting federal aid in his campaign for the presidency, including derisive comments against those who receive government assistance. But he pulled all the stops to pursue federal aid as governor of Massachusetts, even hiring “revenue maximization” contractors to scour federal programs for every possible penny — and using financial schemes to maximize and then divert the aid from his needy constituents.Sphere: Related Content
Medicare IPAB: Rational or rationing? - amednews.com
Medicare IPAB: Rational or rationing? - amednews.com
A reasonable overview of IPAB, in spite of a little alarmist rhetoric at the beginning...
How the board might work
If the IPAB authority is not repealed, the president will appoint members after consulting with Congress. The positions carry a six-year term and a $165,000 annual salary and are subject to Senate approval.
Board members are expected to be experts in health care finance and economics, actuarial science, management, health insurance, integrated delivery systems and payment models, according to a March Congressional Research Service report. In addition, members should have expertise in certain sectors of the health care system, meaning that a doctor, an expert on drug manufacturing, an employer representative, a third-party payer official or a patient advocate could be a nominee. However, the statute states that a majority of members should not be involved directly in providing Medicare services, limiting the participation of practicing Medicare physicians.
The Centers for Medicare & Medicaid Services chief actuary first would decide in 2013 if IPAB actions are needed. The actuary will calculate a Medicare per-capita growth rate and a target rate defined by statute. Starting in 2018, growth targets will be pegged to gross domestic product plus one percentage point.
IPAB would not be required to act as long as program growth remains under that target rate. If it exceeds the target, the board would be required to submit a cost-savings proposal that Congress must consider under special fast-track rules. The proposal would become law unless Congress passes an alternative with the same level of savings or overrides the proposal with a three-fifths vote in the Senate.
Those spending reductions could go into effect as early as 2015, but government actuaries said that is unlikely. The Congressional Budget Office projects that Medicare spending will not eclipse growth targets for years, and thus IPAB won’t be responsible for drafting a savings plan through at least 2021 if expected trends hold.Sphere: Related Content
Sunday, October 14, 2012
What if Medicare’s drug benefit was more like the VA’s? | The Incidental Economist
What if Medicare’s drug benefit was more like the VA’s? | The Incidental Economist
Medicare’s inability to negotiate program-wide prices and tighten plan formularies is in stark contrast to the VA, which negotiates directly with drug manufacturers and is not bound by the same formulary rules as Part D plans. That’s why the VA has been able to implement a national formulary more restrictive than those of Medicare plans and obtains lower drug prices. If Medicare plans could implement VA-like formularies and obtain commensurately lower prices, our paper shows that enough could be saved to compensate beneficiaries for the loss of choice, with savings to spare.
To repeat, the key findings are:
The VA pays 40% less than Medicare plans for prescription drugs.
Medicare plans cover about 85% of the most popular 200 drugs on average (ranging from a low of 68% to a high of 93%).
The VA’s national formulary includes 59% of the most popular 200 drugs.
If Medicare obtained the same drug prices as the VA, it would save $510 per beneficiary per year or a total of $14 billion per year (2009 prices).
If Medicare plans tightened formularies to the level of generosity available from the VA (59% of top 200 drugs covered), beneficiaries would lose $405 of value per year associated with the loss of choice of drugs. (The right way to interpret this is that the average beneficiary would be precisely indifferent between the loss of drug choice and $405 dollars in cash.)
Because the savings ($510 per beneficiary) exceeds the loss of value to beneficiaries ($405), they could, in principle, be made whole with $105 left over (= $510 – $405).
A Possibly Fatal Mistake - NYTimes.com
A Possibly Fatal Mistake - NYTimes.com
But the cancer has kept growing, and I went to the E.R. again on Sept. 17 when I found that I was losing all strength in my legs. They did an M.R.I. and saw that there were tumors pressing on my spinal cord. They have been treating me with radiation for three weeks now to shrink those tumors and will continue to do so for another week.
I submitted an application to the hospital for charity care and was approved. The bill is already north of $550,000. Based on the low income on my tax return they knocked it down to $1,339. Swedish Medical Center has treated me better than I ever deserved.
Some doctor bills are not covered by the charity application, and I expect to spend all of my I.R.A. assets before I’m done. Some doctors have been generously treating me without sending bills, and I am humbled by their ethic of service to the patient.
Some things I have to pay for, like $1,700 for the Lupron hormone therapy and $1,400 for an ambulance trip. It’s an arbitrary and haphazard system, and I’m just lucky to live in a city with a highly competent and generous hospital like Swedish.
Everything Obama has done — and wants to do — on taxes in one post
Everything Obama has done — and wants to do — on taxes in one post
The centrality of tax policy to the 2012 election raises the question: What has actually changed in the tax code since Obama took office?
Three of the big bills of Obama’s tenure — the American Recovery and Reinvestment Act (or the stimulus act), the Affordable Care Act, and the Bush tax cuts reauthorization/payroll tax cut deal from 2010 — contain most of the changes that have been passed since January 2009. Let’s run through them, bill by bill. Keep in mind, of course, that Congress writes the laws, and the bills that actually passed only somewhat reflect Obama’s priorities.Sphere: Related Content
Medicaid's high marks on preventive care contrary to its stingy image - amednews.com
Medicaid's high marks on preventive care contrary to its stingy image - amednews.com
Medicaid, with its reputation for low payment rates and fiscal instability, is far from perfect, said Stacey Mazer, senior staff associate for the National Assn. of State Budget Officers. Budget officers in particular continue to have concerns about the fact that health care spending is outpacing other services.
Kaiser’s findings highlight all of the positive benefits that Medicaid can provide, Mazer said. “The states did very well in terms of the number of preventive services that they covered, and even the states that didn’t cover as many still covered the majority of them.”Sphere: Related Content
Wednesday, October 10, 2012
Bob Cesca: Repeat After Me: Obama Cut the Deficit and Slowed Spending to Lowest Level in 50 Years
Bob Cesca: Repeat After Me: Obama Cut the Deficit and Slowed Spending to Lowest Level in 50 Years
As I've documented before, the CBO reported in January, 2009 that the federal budget deficit for that fiscal year, which began on October 1, 2008, was already $1.2 trillion. President Obama's additional '09 spending added another $200 billion to the deficit, bringing the total to $1.412 trillion. Unprecedented and huge, but given the enormity of the financial crisis and the depth of the recession, there weren't many other options on the table. Add two wars into the mix and there you go.
But since then, deficit spending has dropped precipitously. Why? Chiefly because President Obama signed the Statutory Pay-As-You-Go Act in February, 2010, which mandates that new spending be offset with spending cuts or new revenue. Yes, a Democratic president and a Democratic Congress passed this legislation. Guess how many congressional Republicans voted for the law. Zero. Not one. Perhaps during this week's debate, Vice President Biden could ask Rep. Paul Ryan who voted against the bill.
Consequently, the president is responsible for the lowest government spending growth in 60 years, according to the Wall Street Journal's Market Watch.Sphere: Related Content
Tuesday, October 9, 2012
Wendell Potter: Romney's Phony Answers to Tough Health Care Questions
Wendell Potter: Romney's Phony Answers to Tough Health Care Questions
High on the list of recommendations in Romney's health care platform is an idea frequently touted as a silver bullet by conservatives: allow insurance companies to sell policies across state lines. Doing so, they say, will increase competition and, consequently, bring down the cost of coverage.
The problem is that no one had done a study to determine definitively whether the across-state-lines idea would work -- until now. And the conclusion of that study, conducted by the Georgetown University Health Policy Institute, is that allowing coverage to be purchased across state lines is much more of a blank than a bullet.
The study also finds that no new federal law is even needed to allow insurance companies to sell policies across state lines.
"With or without changes to federal law, states already have full authority to decide whether or not to allow sales across state lines and, if so, under what circumstances," the study noted.
Of course, you wouldn't know that from listening to Romney and other politicians who seem to believe than an act of Congress is needed. It isn't. State legislatures can make it happen whenever they want, but, so far, only six have decided to try it. Georgia, Maine and Wyoming have enacted legislation in recent years to allow out-of-state insurers to sell policies within their borders. Lawmakers in Kentucky, Rhode Island and Washington passed bills requiring their insurance departments to research the idea and determine interest from out-of-state insurers.
The lawmakers who championed the legislation expected their states would be inundated with applications from insurers far and wide eager to sell their policies. But it hasn't happened. In fact, not a single insurance company has expressed the slightest interest in doing business in any of those six states.Sphere: Related Content
Study: When health insurance costs rise, productivity drops
Study: When health insurance costs rise, productivity drops
A new working paper from Truven Healthcare’s Teresa Gibson, Harvard’s Michael Chernew and the University of Michigan’s A. Mark Fendrick find that as co-payments go up, productivity drops — most likely as a result of employees skipping out on care altogether.
The team focused on those with chronic pain such as arthritis. They then looked at how much employees had to pay for prescription medication under their various benefit structures. Previous research has shown that as the cost of health-care services increases, usage decreases — workers simply don’t fill as many prescriptions when prices get higher.
On average, employees with chronic pain had 76.7 hours absent from work. But with every $5 increase in cost-sharing for pain medications, they saw an increase in absenteeism somewhere in the ballpark of 1.3 to 3.1 percent.Sphere: Related Content
Monday, October 8, 2012
Obama's healthcare law: Historic reform and signature failure - latimes.com
Obama's healthcare law: Historic reform and signature failure - latimes.com
His [Obama's] one condition was a healthcare plan that would protect Americans and could pass," said Neera Tanden, a former senior White House health advisor.
Several Republican lawmakers signaled interest in working with Obama. But almost at the outset, the GOP leadership was dug in.
"There were legitimate policy disagreements," said John McDonough, a former aide to the late Sen. Edward M. Kennedy (D-Mass.), "but the clear message we heard from the GOP staffers was they couldn't move without a signal from McConnell."
The Republican Senate leader pressured GOP senators to stop negotiating with Obama. "It was intense and it was constant," said one former Republican aide, who asked not to be identified discussing internal party tensions.
Healthcare leaders got a similar message. One executive said he received several calls from senior GOP lawmakers warning that he would regret participating in the process. Another said he was told that Republicans would not do anything to make the legislation better. "Republicans were going to vote against the law, no matter what," a third executive said.
All three declined to speak publicly for fear of angering GOP congressional leaders.
Despite the hostility, Obama spent most of 2009 pursuing Republican votes.:-(
Sphere: Related Content
Monday, October 1, 2012
I am a job creator: A manifesto for the entitled - The Washington Post
I am a job creator: A manifesto for the entitled - The Washington Post
I am the misunderstood superhero of American capitalism, single-handedly creating wealth and prosperity despite all the obstacles put in my way by employees, government and the media.There's lots more and it is all dead on! Sphere: Related Content
I am a job creator and I am entitled.
I am entitled to complain about the economy even when my stock price, my portfolio and my profits are at record levels.
I am entitled to a healthy and well-educated workforce, a modern and efficient transportation system and protection for my person and property, just as I am entitled to demonize the government workers who provide them.
I am entitled to complain bitterly about taxes that are always too high, even when they are at record lows.
I am entitled to a judicial system that efficiently enforces contracts and legal obligations on customers, suppliers and employees but does not afford them the same right in return.
I am entitled to complain about the poor quality of service provided by government agencies even as I leave my own customers on hold for 35 minutes while repeatedly telling them how important their call is.
I am entitled to a compensation package that is above average for my company’s size and industry, reflecting the company’s aspirations if not its performance.
I am entitled to have the company pay for breakfasts and lunches, a luxury car and private jet travel, my country club dues and home security systems, box seats to all major sporting events, a pension equal to my current salary and a full package of insurance — life, health, dental, disability and long-term care — through retirement.
Bush-Appointed Judge Upholds Obama Administration's Birth Control Coverage Rules | ThinkProgress
Bush-Appointed Judge Upholds Obama Administration's Birth Control Coverage Rules | ThinkProgress
The crux of the argument, from the beginning, is reenforced by the Judge:
[Federal religious freedom law] is a shield, not a sword. It protects individuals from substantial burdens on religious exercise that occur when the government coerces action one’s religion forbids, or forbids action one’s religion requires; it is not a means to force one’s religious practices upon others. [It] does not protect against the slight burden on religious exercise that arises when one’s money circuitously flows to support the conduct of other free-exercise-wielding individuals who hold religious beliefs that differ from one’s own.Sphere: Related Content
Monday, September 24, 2012
Let health reform do its job
Let health reform do its job
A patient loses his insurance and it puts his life at risk. Everyday stuff in America.
Health insurance is essential for living well with chronic disease, and the loss of access to care is a major cause of preventable illness and death, but it is also ultimately much more costly to society than long-term continuous primary care. As a doctor, I know how to help people. I can't do it when I don't see them because they cannot afford to come in. We need to shift our care to the doctor's office and away from the expensive emergency room.
The Affordable Care Act is in the process of correcting that fatal flaw in our health care system. With the benefits for seniors including making medications more affordable and shoring up Medicare, Medicaid expansion, health insurance exchanges (that would help people like Mr. Smith), subsidies to purchase insurance and spreading of risk across large populations to make possible the ending of exclusion for pre-existing conditions, the coverage gap for patients such as mine should ultimately be a thing of the past.
Most medical organizations are supporting the ACA. Most primary physicians favor it as at least a major step toward access to health care. Those who oppose it and work to create barriers to implement it have yet to offer a reasonable alternative that would help patients such as Mr. Smith. If they have one, it is time to tell the American people what they have in mind, and if not, they should step aside and let reform do what it was designed to do.From Doctors for America member Ian Gilson. Sphere: Related Content
Tuesday, September 18, 2012
Romney’s theory of the “taker class,” and why it matters
Romney’s theory of the “taker class,” and why it matters
For what it’s worth, this division of “makers” and “takers” isn’t true. Among the Americans who paid no federal income taxes in 2011, 61 percent paid payroll taxes — which means they have jobs and, when you account for both sides of the payroll tax, they paid 15.3 percent of their income in taxes, which is higher than the 13.9 percent that Romney paid. Another 22 percent were elderly.
So 83 percent of those not paying federal income taxes are either working and paying payroll taxes or they’re elderly and Romney is promising to protect their benefits because they’ve earned them. The remainder, by and large, aren’t paying federal income or payroll taxes because they’re unemployed. But that’s a small fraction of the country.Sphere: Related Content

Friday, September 14, 2012
Mitt Romney Thinks "$200 - $250K or less" is middle income!
Full Transcript: George Stephanopoulos and Mitt Romney - ABC News
GEORGE STEPHANOPOULOS: Is $100,000 middle income?
MITT ROMNEY: No, middle income is $200,000 to $250,000 and less.
Reality:

Ahh, another MBA in the White House. Hooray!
Sphere: Related Content
Sunday, September 9, 2012
RAND Institute for Civil Justice | RAND
RAND Institute for Civil Justice | RAND
Most Physicians Will Face Malpractice Claims, But Risk of Making Payment Is Low
The most comprehensive analysis of the risk of malpractice claims by physician specialty in more than two decades finds that U.S. physicians have a greater than 75% career-long risk of facing litigation. In some specialties, doctors can be virtually certain of a lawsuit over the course of their careers. However, the vast majority of those claims will not result in payment to a plaintiff. Sphere: Related ContentDaily Kos: In defense of red state socialism
Daily Kos: In defense of red state socialism
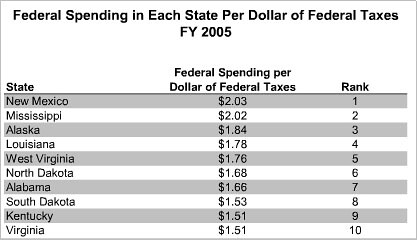
Support for Republican candidates, who generally promise to cut government spending, has increased since 1980 in states where the federal government spends more than it collects. The greater the dependence, the greater the support for Republican candidates.
Conversely, states that pay more in taxes than they receive in benefits tend to support Democratic candidates. And Professor Lacy found that the pattern could not be explained by demographics or social issues.Sphere: Related Content
Thursday, August 23, 2012
JAMA Network Controlling Health Care Costs in Massachusetts With a Global Spending Target
The new legislation builds on the far-reaching health insurance reforms that Massachusetts enacted in 2006, including the mandate on state residents to carry a minimum level of insurance or to pay a tax penalty.6 The reforms became the model for key aspects of the US Patient Protection and Affordable Care Act of 2010.1 The many features of the 2012 state act include provisions to improve transparency and accountability for health care providers with regard to cost, financial performance, quality, and competition within markets and to improve the clarity for consumers of information about the out-of-pocket costs of care. The provisions also include reforms to medical malpractice laws that would allow a physician, hospital, or others who provide health care to admit to a mistake or error, without the acknowledgment being used in court as an admission of liability.5 Attention, however, is likely to focus on the global spending target and its potential value as a cost-containment tool. From 2004 to 2009, health care spending in Massachusetts increased by 5.8% per year, regularly exceeding economic growth.7JAMA Network | JAMA: The Journal of the American Medical Association | Controlling Health Care Costs in Massachusetts With a Global Spending Target Controlling Health Care Costs in Massachusetts Sphere: Related Content
The act creates a Health Policy Commission to implement the new law and a Center for Health Information and Analysis to collect and analyze data on health care costs and quality. The commission is charged with establishing by April 15 of every year “a health care cost growth benchmark for the average growth in total health care expenditures . . . for the next calendar year.” Total health care expenditures are defined as “all health care expenditures in the commonwealth from public and private sources,” including “all categories of medical expenses and all non-claims related payments to providers . . . all patient cost-sharing amounts, such as, deductibles and copayments,” and “the net cost of private health insurance.” The “growth rate of potential gross state product” is defined as the “long-run average growth rate of the commonwealth's economy, excluding fluctuations due to the business cycle.”
Subscribe to:
Comments (Atom)
So, clearly the 47% of moochers are across the political and ideological spectrum, contrary to Mitt Romney's suppositions (fantasies?)